Relative energy deficiency in sport (RED-S) is the result of insufficient caloric intake and/or excessive energy expenditure. Consequences of this low-energy condition can alter many physiological systems, including metabolism, menstrual function, bone health, immunity, protein synthesis, and cardiovascular and psychological health.
It was more commonly known as the female athlete triad, but now RED-S is the term used as it can also be present in men.
However, this article will cover RED-S in women.
The signs and symptoms of RED-S are broad, often mild and therefore miss-attributed to ‘that's just life’ events, often going unnoticed or ignored.
But its important to be aware and catch this syndrome early to prevent potentially long term damage to health and training.
The three main components of RED-S refer to the association between the following three clinical conditions:
Low energy availability (with or without an eating disorder)
Menstrual dysfunction (amenorrhoea)
Low bone mineral density (osteoporosis)
Low energy availability:
This basically means that the woman is not eating enough to meet her daily requirements. It may be related to an ‘eating disorder’ or ‘disordered eating’ of some kind, especially for sports in which leanness and low body weight is encouraged, such as running, dancing, gymnastics or skating. This can then result in low body weight and a very low body fat percentage.
Menstrual dysfunction: The clinical end point of menstrual dysfunction is amenorrhoea (periods stopping for 3 or more months). In the case of low energy availability, menstrual cessation is a survival mechanism. When we have sufficient energy, the brain releases a hormone (gonadotrophin releasing hormone) which stimulates the ovaries to release oestrogen and progesterone, allowing for regular menstrual cycles with the goal of reproduction.
But when there is a lack of energy availability or a low body fat percentage, the body wants to conserve its resources and the last thing the body needs is to spend energy and nutrients on making a baby! This means the brain stops producing hormones to promote secretion of reproductive hormones and menstruation eventually comes to a holt.
Low bone mineral density: The final condition in the triad is lowered bone mineral density, the clinical end point of which is osteoporosis. The key factor here is lack of oestrogen (due to the altered cycle of hormone production, as above), as oestrogen stimulates normal bone mineralisation in women.
Other factors causing lowered bone mineral density can include lack of the necessary bone-supporting nutrients such as calcium, magnesium and fat-soluble vitamins A, D and K in the diet, and lowered oestrogen availability.
BE AWARE
This is a progressive condition stemming from inadequate energy intake. Each component exists on a continuum between health and pathology. This means clinical symptoms of all three may not always be evident together. For example, periods may have changed in regularity or length rather than ceased, and bones may have begun to brittle but are not yet osteoporotic, and evidence of reduced bone mineral density is unlikely to be evident unless tested for or fractures have occurred. It’s important we try to catch this early to prevent any long term irreversible damage.
Are you at risk?
The following are factors which may increase your risk:
Performing in a sport comprising of weight classifications e.g. rowing, weightlifting, boxing.
Sports which historically correlate low body mass and fat to success e.g. triathlons, long distance running, ballet, gymnastics, figure skating.
Simply being in an environment that idolises leanness and/or thinness as something to strive towards.
Current or history of an eating disorder
SIGNS AND SYMPTOMS TO LOOK OUT FOR -
Low energy and general feelings of weakness and fatigue
Poor recovery and repair from training i.e. feeling sore and drained going into and during sessions
Plateau or reduced strength and/or muscle size
Catching coughs, colds and infections more often (decrease immune function)
Lack of sex drive
Depression
Irregular periods/ change in cycle or period length
Increase in injuries
Stress fractures
Restricting eating to certain food groups
Feelings of guilt after eating certain foods or missing training
Impact on health and performance
The ‘triad’ is how the condition is classified, with the health implications travelling along the pathological continuum towards infertility and osteoporosis.
However, the implications and negative outcomes of the female athlete triad can be far-reaching, impacting not only day-to-day performance and wellbeing, but also long-term health. This is why the Female Athlete Triad has now been coined as Relative Energy Deficiency in Sport (RED-S).
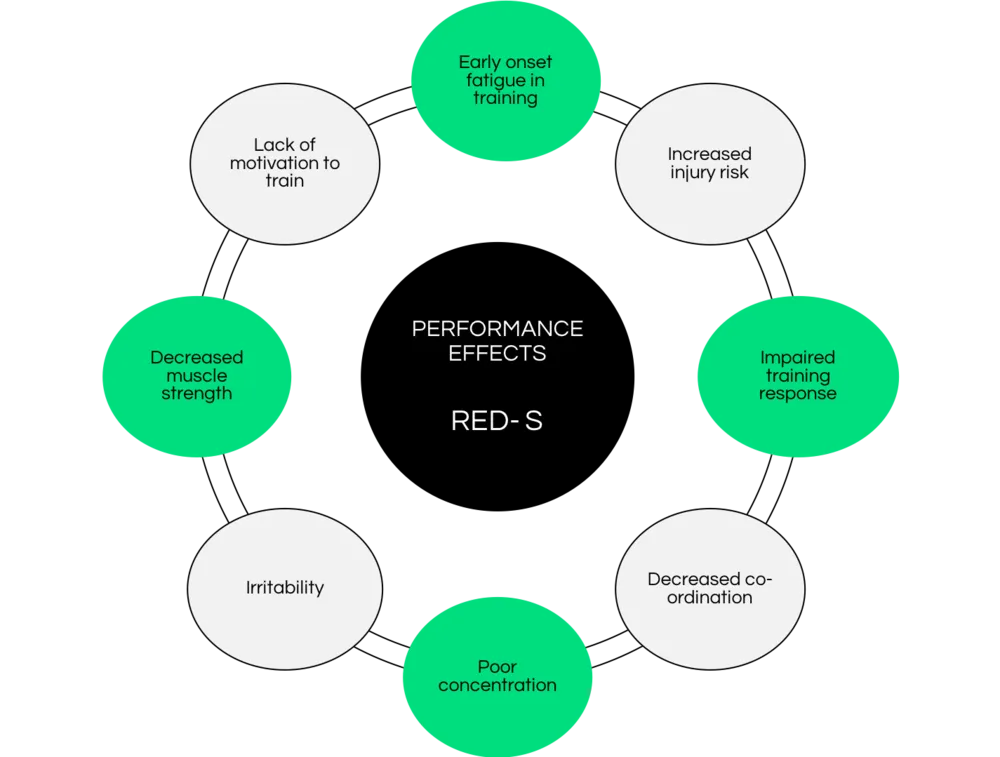
Impact on performance:
Reduced aerobic capacity
Reduced anaerobic (sprinting) capacity
More missed training sessions due to illness
Reduced strength
Early onset fatigue in training sessions
Lack of drive to train
Impact on health:
Increased cardiovascular disease risk
Low thyroid function
Adrenal fatigue
Infertility
Stress fractures and osteoporosis
Mental health issues including anxiety, depression, eating disorders
How to re-balance energy
Addressing low energy availability involves increasing energy intake, reduction in exercise or a combination of both until energy expenditure is met by energy intake.
Step 2: Identify and underlying causes of disordered eating. This could be that you don’t have a structure to when or what you eat and skipping meals. If you are struggling with disordered eating or want help/advice for yourself or someone you care about you suspect of suffering from an eating disorder, please get in contact and we will help guide you to the help and support you need.
Step 3: Recruit support from friends and family. It can be both physically and psychologically challenging to change habits and identify and overcome barriers to increasing food intake or reducing training volume.
Step 4: Address the underlying causes of the low energy availability to allow you to incrementally increase calorie intake per day and consider reducing training volume (i.e introducing a rest day/reducing double training days to single) until energy intake meets daily energy expenditure. These additional calories should come from high quality sources of protein and carbohydrates and be distributed predominantly around training.
Supporting menses (menstrual cycle) and bone health
To avoid menstrual disturbances it is key to ensure energy balance and healthy body fat percentage (this is vital for women to produce oestrogen). Consuming adequate quantities of quality carbohydrates (especially after training) will also aid in supporting proper hormonal regulation.
To maintain healthy bones we want to ensure we are consuming adequate amounts of calcium from food sources and should all be taking a Vitamin D supplement of 1000IU/day. This is especially important throughout the winter months.
If you are concerned that you or someone you know is showing signs or symptoms, please do not hesitate to get in touch with us. Becs our nutrition coach can help answer any of your questions if needed. Drop her an email on becs@phnutrition.co.uk
We have a 4-week eating through your menstrual cycle program including with the hub membership.
Changing your training and food choices around your menstrual cycle is something that can have a real positive impact. However, there is limited advice on how to do it!
This 4-week habit will show you -
The different phases of the cycle
Training considerations in each phase
Nutrition choices for each phase
Key nutrients
Sign and symptoms and how to address them
Use this program to learn about how to structure your nutrition and training around your menstrual cycle.
You also get access to our menstrual cycle recipe pack!!
Keay, N. 2018 UPDATE: Relative Energy Deficiency in Sport (RED-S). British Journal of Sports Medicine Blog. May 2018
Statua, SM., Asif, IM., Drezner, JA. Relative energy deficiency in sport (RED-S). British Journal of Sports Medicine. November 2017 51(21).
Joy, E., De Souza, M., Nattiv, A. et al 2014 Female athlete triad coalition consensus statement on Treatment and return to play of the female athlete triad. August 2014 13(4).